Injuries of the AC joint (the joint connecting the collarbone to the shoulder blade) are among the most common sports and fitness training related injuries. One type of painful shoulder condition is Weightlifter’s Shoulder. Weightlifter’s Shoulder, also called AC joint Osteolysis, or Distal Clavicular Osteolysis (DCO), can affect people whose sports or job activities involve repetitive overhead movements. They may experience shoulder pain that, in some cases, can become increasingly severe. Here is some information about symptoms, diagnosis, treatment and prevention of DCO.
Who is Affected by Weightlifter’s Shoulder?
As you can assume, based on the name, this shoulder problem is most common among power lifters, weightlifters and fitness training enthusiasts. But, people engaged in many other types of activities are susceptible to Weightlifter’s Shoulder. Many athletes, including martial artists, boxers, racquetball players, handball players, rugby players and golfers experience pain from DCO. Air-hammer operators, hair stylists, construction workers, and various types of military members and others whose jobs involve repetitive overhead motions also suffer from this injury.
What is Weightlifter’s Shoulder?
Distal Clavicular Osteolysis, also called AC joint Osteolysis (Acromioclavicular Joint Osteolysis), or Weightlifter’s Shoulder is a painful condition resulting from deterioration of the distal end of the collar bone (clavicle). Overuse through repetitive motion causes tiny fractures along the end of the bone, leading to Osteolysis, which means erosion (deterioration or breakdown) of the bone.
DCO occurs when the bone is becoming eroded at a faster rate than the body can repair or replace it. As the small fractures deteriorate, these erode the bones of the AC joint. Blood vessels form around the area during the body’s attempt to heal. Commonly, the area becomes chronically inflamed with fibrosis (scar tissue). The synovial lining of the joint begins to over-generate itself due to the injury and encroaches on the underlying bone, contributing to healing issues. Left untreated, the pathological process can ultimately lead to degenerative joint disease.
What Parts of the Shoulder are Affected?
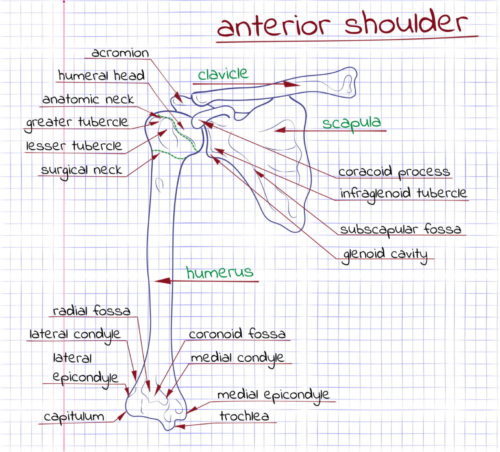
The shoulder consists of three bones, including the collar bone (clavicle), shoulder blade (scapula) and the upper arm bone (humerus). Ligaments and soft tissues hold together and stabilize the AC joint. Ligaments in the area include the superior and inferior AC ligaments, coracoclavicular ligament and the AC joint capsule. A fibrocartilaginous disc is located between the acromion and clavicle, which cushions and helps to convey forces onto the AC joint. Some or all of these bone structures and connective tissues can be affected in cases of Weightlifters Shoulder injury.
What Causes DCO?
Repetitive damage to the AC joint from overhead weightlifting or other types of activities mentioned above causes tiny bone fractures along the distal end of the clavicle. The rate of adding more injury by repeating the injurious activity can exceed the ability of the bone to heal, resulting in DCO.
Excessive impact to the AC joint during chest fly, bench press, dumbbell press and other movements occurs when elbows drop behind or below the body. This places the shoulders in a position of excess extension. Because the bone does not have time to heal before the next weight training session, the injury continues to worsen, and the end of the clavicle bone begins to dissolve.
In the majority of cases of DCO, repetitive stress to, or compression of the AC joint from intensive lifting during workouts or job tasks has led to the orthopedic condition. However, in some cases, the injury can be caused by direct trauma. People with a history of acute injury to the AC joint may experience DCO without incurring any previous trauma to the area.
Symptoms of Weightlifter’s Shoulder
Common symptoms of DCO can include:
- Sensitivity and pain when pressure is applied to the top of the shoulder
- Dull aching around the AC joint
- Swelling in the AC joint or around the end of the collarbone, and possibly spreading to the deltoid or neck
- A general feeling of weakness of the shoulder
- Strong pain in the shoulder later in the day or evening after upper body workouts or other repetitive upper body activity.
How is DCO Diagnosed?
A physical examination along with a review of the patient’s personal medical history are used by healthcare professionals in diagnosing DCO. The doctor or Physical Therapist may move or press the AC joint.
A Scarf Test may also be performed. In this test, the patient may be asked to flex the arm to 90 degrees, then place the hand on his or her opposite shoulder and push back with that hand.
Other diagnostic tools used to identify the condition may include AC joint Osteolysis X-ray, MRI or bone scan of the AC joint.
What is the Treatment for DCO?
For people with Weightlifter’s Shoulder, attempting to work through the pain can lead to worse consequences to your workout and your shoulder condition. So, if you develop DCO, avoid movements such as dips, bench press, push-ups and throwing motions during the weeks of healing. These can make symptoms worse and negatively affect the recovery process.
Weightlifter’s Shoulder usually responds well to a conservative treatment plan of rest and rehabilitation. Such treatment usually includes:
- Avoiding heavy lifting for a few weeks
- Routinely icing the affected shoulder area
- Anti-inflammatory medications (NSAIDs), as recommended by your doctor
- Corticosteroid injections in the AC joint, to relieve pain during bone recovery
- Physical therapy
During treatment, your Physical Therapist (PT) will recommend light therapeutic upper body exercises and encourage you to maintain a cardio routine and other exercises for overall fitness during your recovery from the injury.
The conservative treatment approach is typically suitable for patients who haven’t incurred structural damage to the bone, muscle, or connective tissues. This approach is appropriate for patients who can be expected to recover in a relatively short period of approximately six to eight weeks with this level of treatment. For most patients, painful symptoms gradually disappear as the condition improves, and they can resume all normal activities without a recurrence of the problem.
Stop smoking, because smoking reduces the amount of oxygen that is available to bones and tissues, which leads to less resilient tissue. Also, you may need to avoid lying on the injured side to prevent negatively impact sleep that is needed for optimum healing.
Surgery and Recovery from DCO
For some patients with more severe DCO, the pain is not resolved through conservative treatment, or they are not able to resume their normal activities. In these cases, treatment by an Orthopedic Surgeon may be required to remove (resect) part of the end of the clavicle bone. Treatment can usually be performed using a minimally invasive arthroscopic surgery called AC Joint Arthroplasty (also known as the Mumford procedure).
Minimally invasive arthroscopic surgery is a procedure performed through small pinholes using a narrow instrument. The procedure involves removing less than a centimeter of bone matter from the end of the clavicle and contouring the AC joint. The result is that bones in the AC joint will not grind against one another, which alleviates shoulder pain and enables full range of motion.
Recovery time from the minimally invasive arthroscopic procedure is much shorter than after open surgery. The majority of patients return home the same day. After keeping your arm at rest in a sling for a few days, you will probably be able to begin physical therapy. Any pain or remaining discomfort from surgery usually subsides within several weeks. Most patients fully recover within six to eight weeks in physical therapy.
Prognosis — For weightlifters who follow their doctor’s and physical therapist’s recommendations for treatment and recovery from DCO, there are usually no long-term effects from the injury. However, if proper medical advice is not followed, the injury is much more likely to recur.
How to Prevent Weightlifter’s Shoulder
For weightlifters, preventing DCO can involve making changes in exercises on your weight training routine and/or modifying techniques for execution of upper body movements. Your personal trainer should be able to provide assistance, to ensure that you’re using a proper heavy-light, upper-lower, front-back or other split routines for body building or power lifting.
Technical Modifications to Your Workout — Your trainer should also provide technical guidance throughout your workouts as necessary to ensure proper form, range of motion, speed of movement, and other weight training fundamentals, to avoid DCO as well as other common injuries from weightlifting. A few helpful modifications you can make to some of your movements include:
- Narrow the space between your hands on the barbell, to reduce stress on your distal clavicle.
- Limit your range of motion on your bench press by stopping two inches above your chest, to reduce distal clavicle stress. Try using a two-inch folded towel on the chest to help you control consistency of limiting your motion.Any benefits sacrificed by stopping short of the fullest range of motion are compensated in protecting yourself from a worsening painful condition that can increasingly impact your ability to continue with your upper body weight training routine.
- Modify your techniques for the jerk movement in your clean and jerk power lift set. Instead of racking the bar (lifting the bar and letting it rest on your deltoids or clavicles), start with your elbows approximately even with your shoulders, and lift from there. That eliminates the power pull.
Avoiding Muscle Strength Imbalances — Weightlifters tend to develop stronger chest and anterior shoulder muscles than back muscles and posterior shoulders. Imbalance between strength of these muscles can lend to excessive pressure on the distal clavicle, and lead to development of Weightlifter’s Shoulder.
Your weight routine should rotate between movements that help prevent development of such imbalances in muscle strength. The ratio of lifting movements for chest and anterior shoulder muscles must not exceed the amount of work that is necessary to balance strength in the back and posterior shoulder muscles.
Some muscles may have developed too much strength in contrast to those that serve to neutralize or stabilize them during movement. Your Physical Therapist can evaluate the range of motion and strength of your chest, back and front and back shoulder muscles, to determine whether or not some muscles have been developed to levels of too much strength and what remedial program is necessary.
Strength imbalances of muscles around the shoulder can also arise due to connective tissues that are excessively tight. Your PT will also assess the need for stretching and flexibility routines to remedy this problem.
Chris Keith, Personal Trainer, San Diego
Chris Keith is San Diego’s leading personal fitness trainer. He is widely recognized for his expert guidance in nutrition, flexibility, mobility, weight management, and programs for all levels of athletic development, from beginning to advanced. Chris earned his certification as a fitness trainer during his military service. Over his 25-year career, he has received many awards for excellence in fitness training and has been featured in numerous magazines, newspapers and TV interview programs.
For More Information
For more information about prevention and treatment of Weightlifter’s Shoulder, or about personal weight training programs, contact Chris Keith, Personal Fitness Trainer in San Diego at 619-869-1205, to discuss your personal fitness training goals.